Few individuals with agnosia regain sensory functioning but most make gains within the first few months or year of diagnosis (Rogers, n.d.). There is no specific treatment of agnosia but when possible, the cause of the agnosia is often treated. In other words, damage to regions of the affected cerebrum is treated (e.g., surgery for a stroke). However, most of the time because there is damaged to the brain, there is not much medicinal treatment to be done, especially when the damage is irreversible. Interventions tend to focus on helping individuals with agnosia cope with their condition. Several case studies surrounding agnosias exists in the literature. Treatment principles in these case studies include rehabilitation revolving around repetitive training of impaired function and compensation with utilization of spared function to compensate for the deficit (Ghadiali, 2004). Occupational therapy (OT) is often involved with providing strategies to help individuals with agnosia and his or her caregivers cope and adapt. Hence, the goal of treatment and OT is to develop remedial and compensatory approaches to enable the individual with agnosia to function independently within their context. The following aresome general OT strategies to help accomplish this goal.
Perform tasks in predictable environments (Rai & Kline, 2004): e.g. place a set of clothes on the same place every morning
De-clutter: e.g. place commonly used items out for use
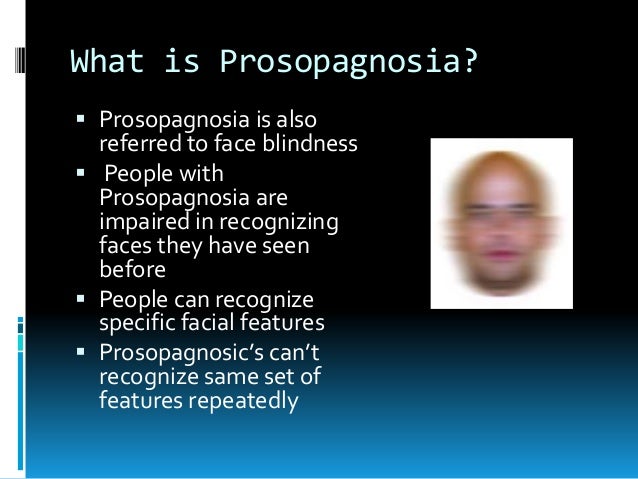
Provide verbal cues: e.g. encourage individuals with prosopagnosia to use a birthmark or facial feature to recognize loved ones
Develop a routine in order to develop consistency in task stimuli
Burns (2010) suggests the following strategies:
o Use Alternative Cues
– Individuals with prosopagnosia can use distinct facial characteristics such as hair style to improve recogniton
– Learn to use contextual information or information revealed during a conversation
– Tactile markers with differing textures can be used in the environment to signify dangerous objects
o Use Alternative Strategies
– Writing down what others say may help an individual with pure word deafness understand a verbal direction or communication; lipreading can also aid in comprehension
– Individuals with alexia can learn to read fairly well through lettertracing
– Teaching an individual with visual object agnosia to feel an object can assist in recognition
o Organizational Strategies
– Organization of clothing using clearly labeled drawers, cabinets, or storage can help making dressing choices easier
– Organization of prepared food so that the individual with agnosia knows where the foods will always be found
– Objects that are used together can be kept in drawers with labels,tactile cues, or colour codes so the individual with
– agnosia knows what each drawer contains

Disclaimer: Research on the use of interventions for agnosias were difficult to come across in the literature, especially auditory and tactile agnosias. In addition, controlled treatment studies with individuals with agnosia are rare. There are, however, several case studies on visual forms of agnosias in the literature. Nevertheless, strategies and interventions are not discussed in depth within these studies. The databases of PubMed, Google Scholar, and Western University library’s Summon feature were utilized using keywords “agnosia” AND “rehabilitation” OR “intervention” OR “treatment” for this search. More research needs to be conducted on general interventions for agnosias.

Any form of agnosia is likely to hinder an individual’s engagement in their day to day activities. Occupational performance issues vary depending on the type of agnosia experienced. Generally, however, the inability to recognize various stimuli can cause issues relating to the person, their occupation, and environment (using the outline of the Canadian Model of Occupational Performance and Engagement). In regards to an individual’s occupation, recognition deficits can lead to occupational performance issues with self-care, productivity, and leisure. For self-care, individuals may need help with eating because they cannot recognize a spoon and fork and as a result use a knife to eat instead (e.g., using a knife to eat a bowl of soup). Grooming can also be difficult if the individual cannot recognize a comb and the purpose of a com Others may need to leave their employment because they are unable to recognize their work setting or carry out previously familiar productivity tasks. There can be occupational performance issues with schooling because of an inability to recognize environmental sounds, such as a school bell, for individuals with nonverbal auditory agnosia. In addition, those with prosopagnosia can have difficulties with recognizing faces of teachers and fellow students, which can lead to hindering of social relationships. A decrease in leisure pursuits may also occur because recognition deficits can lead to difficulty in sustaining participation in leisure activities and as a result decrease engagement in previous enjoyed activities. It is important to note that since memory skills are generally intact for individuals with agnosia, these individuals can still navigate their way around even though they are unable to recognize all the objects or sounds they encounter.
ADAPTED: